Oronasal Fistula
Etiology and Pathophysiology
An oronasal fistula represents a pathological communication between the oral cavity and nasal passages. The most common cause in dogs is advanced periodontal disease, particularly involving the maxillary canine teeth, where progressive alveolar bone loss leads to perforation of the thin palatal bone separating canine tooth socket from the nasal cavity. Other causes include iatrogenic trauma during tooth extraction, not suturing or inappropriate suturing of the extracted canine tooth socket, maxillofacial fractures, penetrating injuries, neoplasia, and congenital defects.Chronic inflammation and bacterial contamination of the nasal cavity perpetuate local tissue breakdown, making spontaneous closure unlikely.
Clinical Signs and Diagnosis
Affected animals commonly present with chronic sneezing, unilateral or bilateral nasal discharge, epistaxis, halitosis, and regurgitation of food or water through the nostrils. Definitive diagnosis is achieved through careful oral examination under anesthesia, probing of suspected defects, and imaging such as dental radiography or cone beam computed tomography (CBCT) to assess the extent of bony loss.
Surgical Treatment
Surgical repair is the treatment of choice and requires meticulous soft tissue handling. The fistula margins must be debrided to healthy tissue, and closure must be tension-free to prevent dehiscence. Common techniques include single-layer buccal mucoperiosteal advancement flaps, rotational flaps, or double-layer flaps in larger defects. Preservation of vascular supply is critical. Postoperative management includes soft diet, prevention of oral trauma, and antibiotic therapy when indicated.
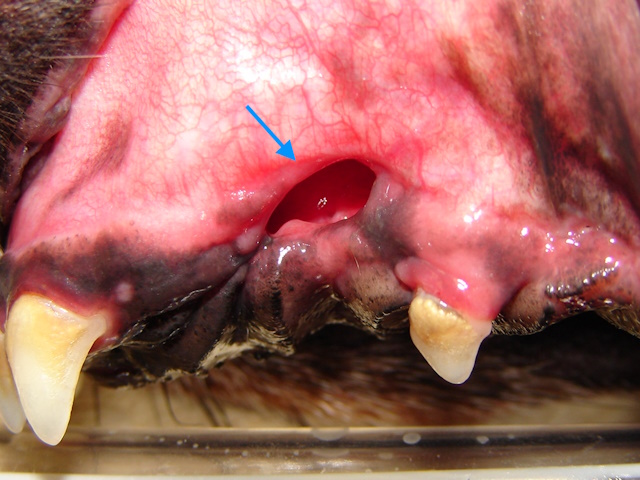
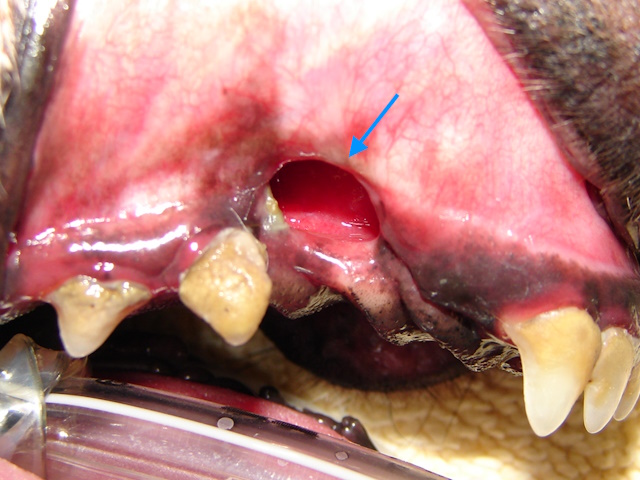
In this Dachshund breed dog, due to significant periodontal disease and bone loss, both left and right upper canines fell off, leaving openings in the mouth that communicate with the nasal cavity (oronasal fistulas).


Both oronasal fistulas were surgically corrected using single-layer buccal mucoperiosteal advancement flaps.
Dentigerous Cysts of the Jaw Bone
Etiology and Pathogenesis
Dentigerous cysts are cysts within the jaw bones that arise from the epithelium layer that surrounds the unerupted teeth. They are most commonly associated with impacted mandibular first premolars in dogs and occur less frequently in cats. Continued secretion of cystic fluid leads to progressive expansion and destruction of the jaw bones by pressure necrosis induced by the continuously increased fluid build-up in these cysts.
Clinical and Diagnostic Features
Many dentigerous cysts are clinically silent until significant bone destruction occurs. Clinical signs may include facial swelling, tooth displacement, pathologic fractures, or delayed eruption. Radiographically, they appear as well-defined, radiolucent (dark appearing) areas surrounding the crown of an unerupted tooth.
Surgical Management Definitive treatment involves surgical removal of the cyst and extraction of the associated unerupted tooth along with teeth that have roots within the cyst cavity. These teeth may have compromised periodontal structures and blood flow. Complete removal of the cyst lining by curettage is essential to prevent recurrence. In large defects, regenerative techniques such as bone grafting or guided tissue regeneration may be considered. Prognosis is excellent with complete excision.
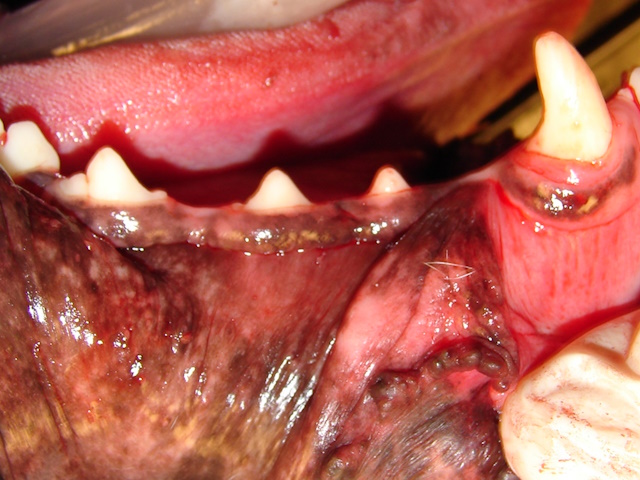
Clinical appearance of the right mandible of a Boxer dog. Notice the first mandibular premolar behind the canine is missing.
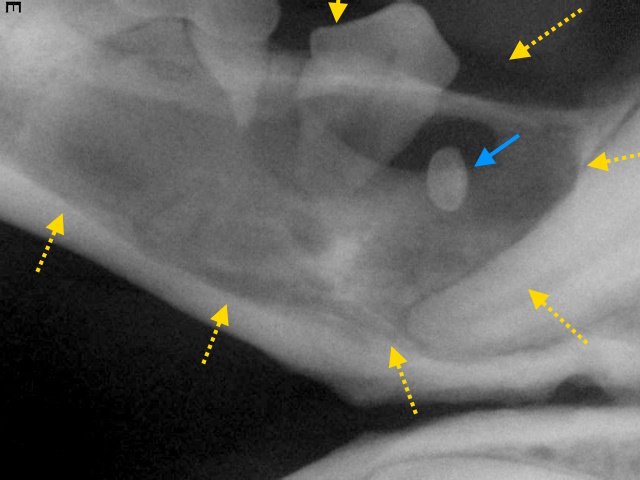
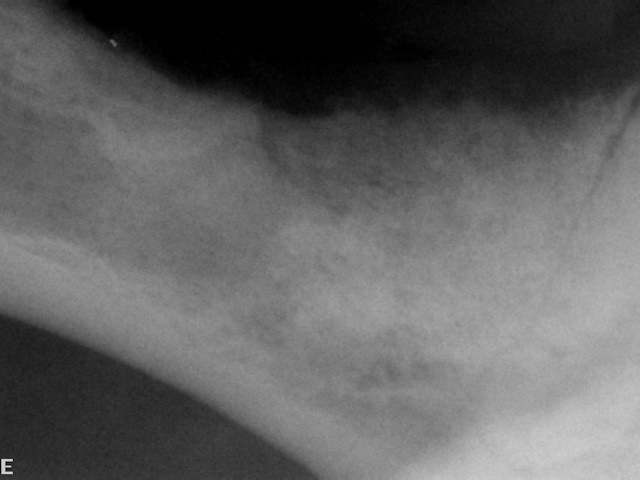
Dental radiograph of this area reveals the small, disfigured mandibular first premolar (blue arrow) inside a large bone cyst (highlighted by the yellow arrows).

The cyst is surgically opened, impacted first premolar and affected second and third premolars were extracted. Cyst lining is completely removedby curettage, and a bone graft was applied in the cavity. Surgical site was sutured and closed.

Dental radiograph of the area after surgery shows complete drainage of the cyst and the applied bone graft for rapid regeneration of the bone in this area.

Three months after the surgery, the surgical site looks clinically well healed.
Dental radiographs show new mandibular bone growth filling the cyst cavity.
Furcation Cysts
Etiology and Pathophysiology
Furcation cysts in dogsare newly identified types of odontogenic cysts linked to severe periodontal disease, causing bone loss where tooth roots meet (the furcation), often appearing near the upper fourth premolar tooth in the dog, and believed to arise from chronic inflammation, infection, or even developmental issues like enamel projections, making them unique inflammatory cysts distinct from typical dentigerous cysts or simple bone cysts.
Clinical Presentation and Diagnosis
Gingival swelling is the most common clinical finding, typically presenting as a soft, fluctuant mass involving the buccal gingiva and overlying mucosa directly adjacent to the maxillary fourth premolar. When the lesion is located superficially, the swelling may exhibit a characteristic bluish discoloration beneath the gingival tissue. Despite the presence of the lesion, the associated tooth often appears clinically healthy and remains vital, which distinguishes this condition from other dental cysts commonly associated with nonvital or fractured teeth. Additional signs of periodontal involvement may be noted, including halitosis, gingival bleeding or enlargement, and visible calculus accumulation near the furcation region.
Surgical Treatment
Treatment of canine furcation cysts is primarily surgical and aimed at complete elimination of the cyst while restoring local oral health. The standard approach involves surgical removal of the cyst lining followed by thorough curettage of the surrounding bone to minimize the risk of recurrence. Although the associated tooth, most commonly the maxillary fourth premolar, is often clinically healthy and vital, extraction is frequently required to allow adequate access and ensure complete removal of the lesion. In more extensive cases, en bloc resection of the tooth and adjacent alveolar bone may be necessary. For very large cysts, a staged approach such as marsupialization can be used initially to decompress the lesion and reduce its size prior to definitive excision. When tooth preservation is attempted, advanced periodontal techniques such as guided tissue regeneration may be considered to address furcation bone loss, although outcomes are variable.
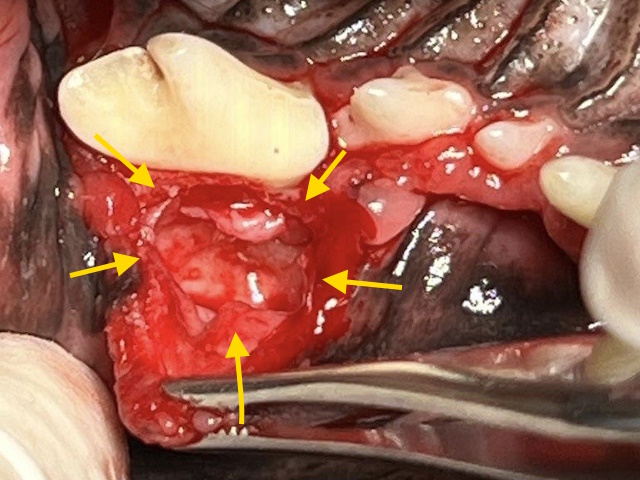
A cyst was identified next to the maxillary fourth premolar tooth (yellow arrows) consistent with a furcation cyst.
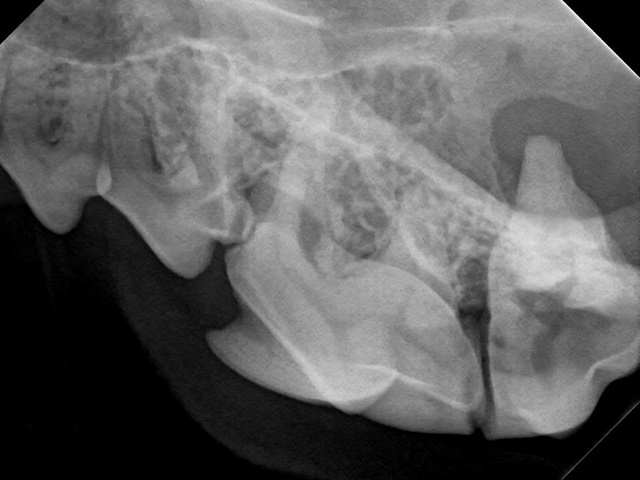
On dental radiograph it was hard to see the cyst, since it was not too big. But a periapical lesion is seen around the palatal root of first molar tooth.
Sublingual Granulomas
Etiology and Pathogenesis
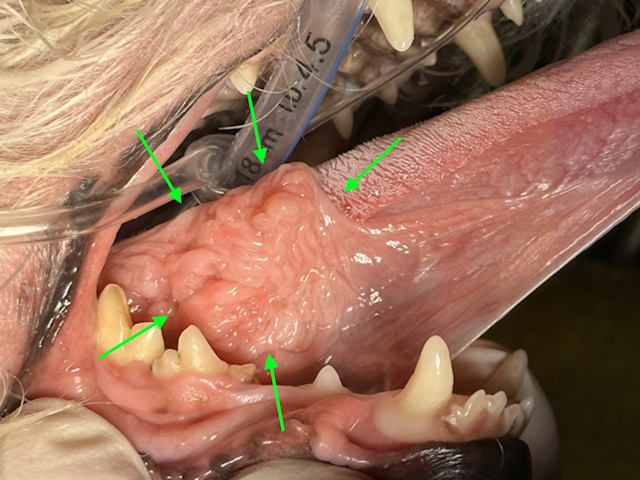
Sublingual granulomas in dogs, often referred to as “Gum-Chewer Syndrome,” are primarily caused by chronic, self-inflicted mechanical trauma. This occurs when a dog repeatedly chews or bites on the loose sublingual mucosa (the tissue under the tongue) or the buccal mucosa (inner cheek lining). Once the initial injury occurs, the tissue becomes inflamed and hyperplastic (enlarged), which unfortunately makes it even easier for the dog to continue biting the same spot during normal mastication.
Clinical Signs and Diagnosis
Clinical signs typically involve visible oral discomfort and the presence of slow-growing, proliferative masses under the tongue. Owners may notice their dog mouth chattering, vocalizing in pain while eating, or dropping food. The lesions themselves often appear as firm, raised, and sometimes ulcerated nodules that can be bilateral (occurring on both sides). In advanced cases, the significant tissue enlargement may be accompanied by hemorrhage or secondary infection. Because these granulomas are often non-painful in early stages, they are frequently discovered during routine sedated oral examinations before behavior changes are noted.
Surgical Management
The primary treatment for sublingual granulomas is the surgical resection of redundant, hyperplastic tissue. Removal of too much of the sublingual fold should be avoided. In cases where the condition is driven by malocclusion or specific teeth irritating the tissue, extraction of the offending teeth may be necessary to prevent recurrence. Post-operative care typically involves soft food and monitoring to ensure the “gum-chewing” habit does not return as the site heals.
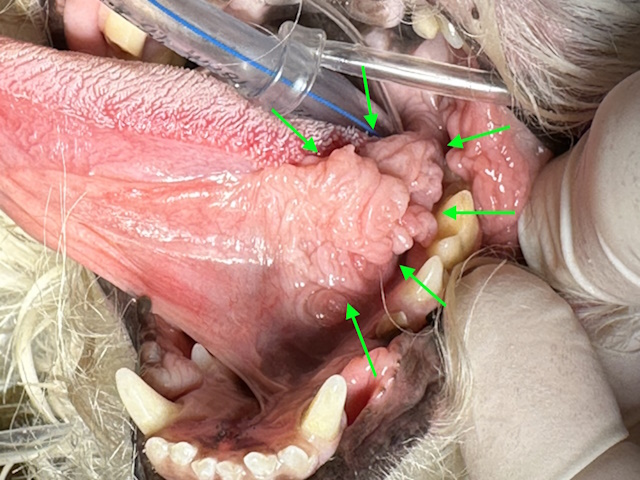
A proliferative mass under the tongue on the left side.
A proliferative mass under the tongue on the right side.
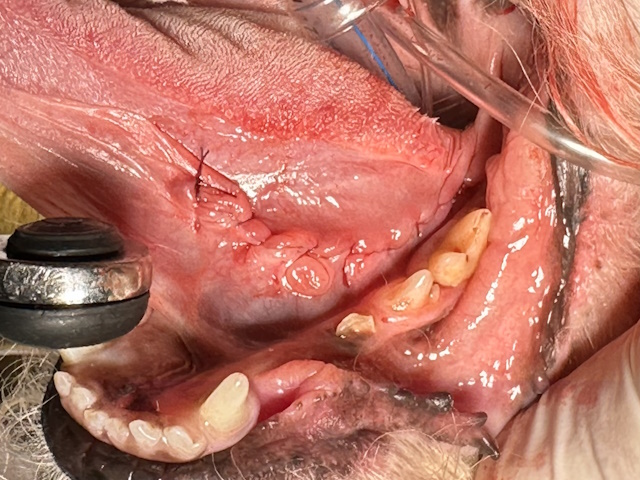
After surgical resection of the proliferative mass.

After surgical resection of the proliferative mass.
Severe Glossitis
Etiology and Pathophysiology
The etiology of severe glossitis in dogs and cats is diverse, often arising from mechanical or chemical trauma, such as chewing on electrical cords, licking caustic substances, or ingesting sharp foreign objects like wood chips or plant burrs. In cats, viral agents—specifically feline calicivirus and herpesvirus—are primary drivers of chronic lingual inflammation and ulceration. Systemic metabolic disorders, particularly uremia from kidney failure, can also trigger severe glossitis by allowing toxins to accumulate and cause oral sloughing.
Clinical Features and Diagnosis
The clinical signs of severe glossitis generally manifests as halitosis, excessive drooling, and a marked reluctance to eat. Animals with severe glossitis may have a visibly swollen, reddened tongue that may develop deep fissures, ulcers, or a dark, foul-smelling discharge. In cats, this pain often results in an “approach-avoidance” behavior where the pet approaches food in hunger but hisses and runs away upon the first attempt to eat. Owners might also observe blood-tinged saliva, pawing at the mouth, or swelling of the regional lymph nodes under the jaw. Diagnosis is based on examination and histopathology.
Surgical Treatment
Treatment options for severe glossitis prioritize addressing the underlying trigger, such as surgically removing foreign bodies or managing systemic kidney disease, alongside supportive care like soft diets, intravenous fluids, and antiseptic mouthwashes. Pain management and antibiotics are essential for secondary infections. Partial glossectomy or focal excision is indicated for severe or refractory cases. The tongue’s rich vascular supply allows for rapid healing, but meticulous hemostasis is essential. Most animals adapt well to partial tongue resection with minimal long-term functional deficits.


Severe ulcerative glossitis on both sides of the tongue in a 8-year-old Cocker Spaniel dog.


Pictures taken immediately after removal of the glossitis lesions from both sides of the tongue.


Remarkable healing of both sides of the tongue after 30 days postoperatively.
Lip Avulsion
Etiology and Clinical Presentation
The etiology of lip avulsion (or degloving) in dogs and cats is predominantly rooted in significant orofacial trauma that applies strong caudally or laterally directed shearing forces against the lips and chin. In dogs, the most frequent cause is animal bites, often from conflicts with other dogs, which frequently result in bilateral rostral upper lip avulsions. In cats, vehicular trauma is the leading trigger, commonly causing the lower lip to be dragged and torn from the mandible at the gingiva or mucogingival junction. Other documented causes across both species include falls from heights, and entrapment in objects like fan belts.
Clinical signs of lip avulsion are typically unmistakable, presenting as a visible separation of the lip or chin from the underlying jawbone, which often exposes the mandible or incisive bone. Owners may notice blood-tinged saliva, excessive drooling, or a foul odor if a secondary infection has developed. Concurrent injuries are highly frequent, occurring in over 80% of cases; these include tooth fractures—most commonly the canine teeth—mandibular symphyseal separation, and traumatic brain injury.
Surgical Repair
Treatment for lip avulsion prioritizes surgical restoration, as healing by second intention often leads to severe tissue contracture and long-term bone exposure. The standard protocol involves thorough debridement of necrotic tissue followed by copious lavage with sterile saline to reduce bacterial load. Surgical repair typically employs tension-free appositional closure using absorbable monofilament sutures. For severe cases with insufficient tissue, advanced techniques are used, such as drilling intraosseous guide holes in the mandible for suture anchorage to relieve shear forces on the healing site.

Lower lip avulsion with proliferative infected soft tissue (indication of chronicity) in a cat.

Healing after surgical correction in 3 weeks. Incisors were extracted for better tissue apposition.
Cleft Palate
Etiology and Pathogenesis
The etiology of cleft palate in dogs and cats is predominantly congenital, occurring when the two halves of the skull or the soft tissues of the mouth fail to fuse properly during embryonic development. Genetic predisposition is considered the primary cause, especially in purebred and brachycephalic breeds like French Bulldogs, Pugs, and Siamese cats. However, environmental factors such as maternal exposure to certain medications, nutritional imbalances, and viral infections during gestation can also trigger the defect. While less common, acquired clefts can occur later in life due to severe orofacial trauma, burns, or advanced periodontal disease.
Clinical Signs and Diagnosis
Clinical signs are often recognized immediately after birth or when nursing begins, most notably as milk bubbling or leaking from the nostrils. Affected neonates struggle to create the negative pressure required for suckling, leading to weak nursing, gagging, and coughing during feeding. Over time, this results in malnutrition, stunted growth, and a general “failure to thrive” compared to littermates. A critical complication is aspiration pneumonia, caused by milk or food entering the lungs, which manifests as respiratory distress, lethargy, and fever. While primary clefts (affecting the lip) are visible externally, secondary clefts (affecting the roof of the mouth) may only be detectable through a thorough oral examination.
Surgical Management
Treatment options for cleft palate focus on definitive surgical repair. Neonates are typically managed with hand-rearing or orogastric tube feeding to ensure adequate nutrition and prevent further aspiration until they are old enough for anesthesia. Surgical correction, or palatoplasty, is generally recommended between 3 and 5 months of age, when the oral tissues have matured. Various flap techniques are used to close the defect without tension. Post-operative recovery is intensive, often requiring a soft diet or feeding tubes for several weeks and strict prevention of chewing to protect the delicate surgical site.
Osteomyelitis
Etiology and Pathophysiology
Maxillary and mandibular osteomyelitis in dogs and cats most commonly arises as a secondary complication of chronic dental and periodontal disease, particularly from infected tooth roots, endodontic disease, or advanced periodontitis that allows bacteria to penetrate the alveolar bone. Traumatic causes such as bite wounds, fractures, penetrating foreign bodies, or iatrogenic contamination following dental extractions or oral surgery can also introduce infection into the bone. Less commonly, osteomyelitis may develop secondary to neoplasia, radiation therapy, or hematogenous spread of bacteria from distant sites, particularly in immunocompromised patients. The condition is typically polymicrobial, involving a mixture of aerobic and anaerobic oral bacteria, and is exacerbated by poor local blood supply and the presence of necrotic bone.
Clinical Signs and Diagnosis
Clinical signs of maxillary and mandibular osteomyelitis vary depending on the location and severity of disease but often include facial swelling, oral pain, halitosis, draining tracts along the face or gingiva, and loose or missing teeth. Animals may show reluctance to eat, dysphagia, or weight loss due to discomfort. Maxillary involvement can result in nasal discharge, epistaxis, or sneezing if infection extends into the nasal cavity or maxillary sinus, while mandibular osteomyelitis may lead to mandibular instability or pathologic fracture in advanced cases. On oral examination, exposed bone, gingival ulceration, or purulent discharge may be observed, and chronic cases may show facial asymmetry or deformity.
Surgical Treatment Management of maxillary and mandibular osteomyelitis requires a combination of aggressive surgical intervention and prolonged antimicrobial therapy. Surgical treatment focuses on removal of the underlying source of infection, including extraction of diseased teeth and thorough debridement of necrotic and infected bone until healthy, bleeding bone is encountered. Removal of dead (necrotic) bone devoid of blood supply (sequester) is often necessary in chronic cases. Culture and sensitivity testing of bone or purulent material should guide antibiotic selection, with therapy typically continued for several weeks to months. In cases with significant bone loss or instability, surgical stabilization may be required. Prognosis depends on the extent of disease and the ability to achieve complete removal of infected tissue.

Necrotic bone around the upper right canine and first premolar teeth.

Examination of the bone with surgical exploration revealed more dead bone under the gumline around the canine and premolar teeth so these teeth were extracted and all the necrotic dead bone was debrided.

Healing of the area after two weeks.

Healing of the area after 5 weeks.