FELINE ORAL AND DENTAL DISEASES
Feline Periodontal Disease
Feline periodontal disease is a progressive inflammatory condition affecting the supporting structures of the teeth and is initiated by the accumulation of bacterial plaque on tooth surfaces. Plaque-induced gingival inflammation, if left untreated, leads to calculus formation, periodontal ligament destruction, alveolar bone resorption, and periodontal pocket development. The host immune response plays a significant role in disease severity, with age, inadequate oral hygiene, concurrent dental conditions such as tooth resorption, and systemic disease contributing to progression. Early disease presents as gingivitis with gingival redness and bleeding, while advanced cases result in gingival recession, tooth mobility, pain, and eventual tooth loss. Severe periodontal disease may lead to oronasal fistula formation, osteomyelitis, and systemic inflammatory effects. Treatment is based on disease severity and includes professional dental cleaning under general anesthesia, periodontal therapy when appropriate, and extraction of teeth with advanced attachment loss. Prognosis is good with early intervention, while advanced disease often necessitates extractions to restore comfort and quality of life.

Significant periodontal disease around mandibular canines and incisors presenting with deep pockets, gum recession and tooth mobility.

Maxillary canine tooth of this cat appears extruded due to chronic periodontal disease. The tooth appears longer than normal with a significant amount of root exposure.
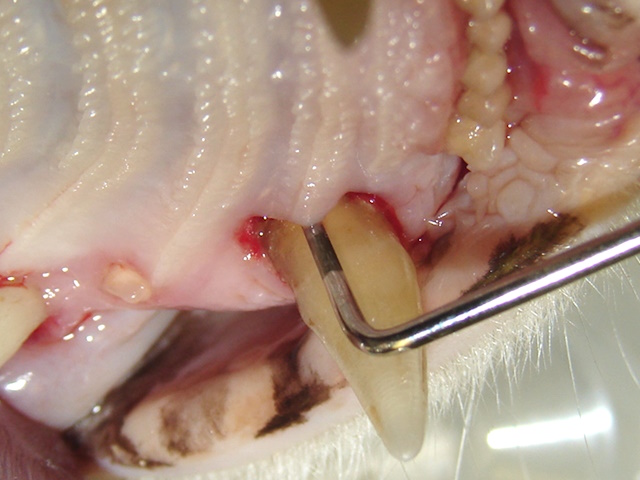
Deep periodontal pocket on the palatal surface of the upper canine.

Gum recession and root exposure affecting the upper third and fourth premolar teeth.
Feline Tooth Resorption
Feline tooth resorption is a highly prevalent, painful, and progressive dental disease characterized by odontoclastic destruction of tooth structure. Although the exact cause remains unknown, inflammatory mediators, altered calcium metabolism, and genetic factors are suspected contributors. Lesions typically originate at or below the cementoenamel junction and progress until structural failure occurs. Clinical signs include oral pain, hypersalivation, gingival inflammation, behavioral changes, and reluctance to eat. Diagnosis relies heavily on dental radiographs, as lesions frequently extend below the gingival margin. The AVDC classifies tooth resorption into Type 1, Type 2, and Type 3 based on radiographic appearance. Type 1 lesions retain normal periodontal ligament space and require complete extraction, while Type 2 lesions exhibit root replacement by bone and are treated with crown amputation when no concurrent disease is present. Type 3 lesions require a combined approach. While affected teeth have a poor prognosis, cats typically show marked improvement following appropriate treatment, though lifelong monitoring is necessary due to the risk of new lesions.

Lower third premolar tooth affected by tooth resorption.

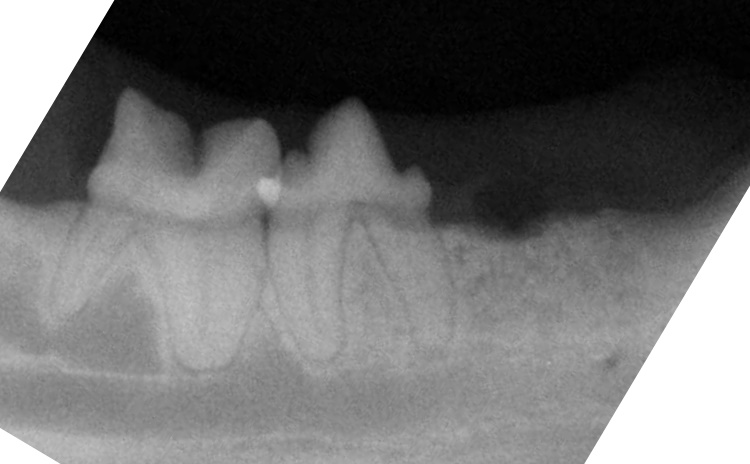
Another cat with lower third premolar tooth affected by tooth resorption.
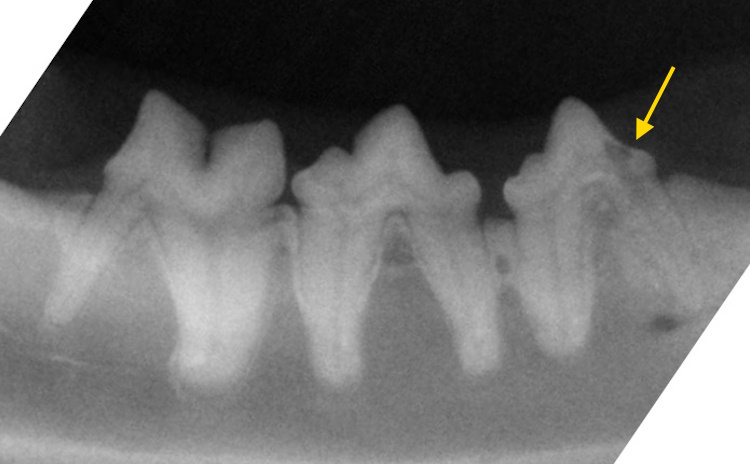
Resorptive lesion can be seen on the crown and neck of the tooth. This is a Type 1 lesion (the root appears normal, and periodontal ligament space is still observable).

This tooth is severely affected by resorptions. This is a Type 2lesion (exhibiting root replacement by bone with no clearly observable periodontal ligament space).

This tooth was treated with complete extraction.
This tooth was treated with crown amputation.
Feline Chronic Gingivostomatitis
Feline chronic gingivostomatitis is a severe immune-mediated inflammatory disease characterized by an exaggerated response to dental plaque and oral antigens. Viral infections, particularly feline calicivirus, along with genetic and immune dysregulation, play a significant role in pathogenesis. Inflammation extends beyond the gingiva to involve caudal oral tissues, resulting in severe pain, dysphagia, weight loss, hypersalivation, halitosis, and behavioral changes. Oral examination reveals marked erythema, ulceration, and proliferative inflammation. Treatment centers on aggressive dental management, with full-mouth or near full-mouth extractions providing the best long-term outcome in most cases. Adjunctive medical therapy may include analgesics, immunomodulatory drugs, and supportive care. Approximately 60–80% of cats show significant improvement following extractions, though some require ongoing medical management. Despite its chronic nature, many cats achieve acceptable long-term quality of life.

Severe oral inflammatory changes consistent with feline chronic gingivostomatitis (FCGS).

Six months after full-mouth extractions, this patient’s mouth is free of inflammation and infection.
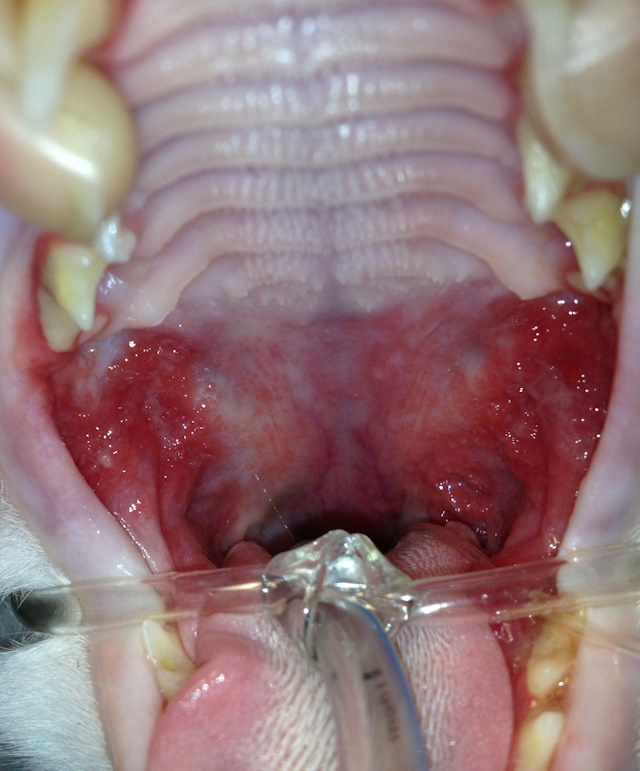
Severe caudal stomatitis. The palatoglossal arches and caudal oral mucosa are intensely erythematous, thickened, and irregular.

Six months after full mouth extraction. Severe caudal stomatitis has resolved and patient has been eating well.
Feline Hyperplastic Juvenile Gingivitis
Feline hyperplastic juvenile gingivitis is an inflammatory condition affecting young cats during permanent tooth eruption and is associated with an exaggerated response to plaque and erupting teeth. Gingival tissues become enlarged, inflamed, and prone to pseudopocket formation, particularly around premolars and molars. Clinical signs include gingival overgrowth, bleeding, halitosis, and oral discomfort, without significant caudal oral involvement. Management focuses on professional dental cleaning, plaque control, and home dental care. Gingivectomy may be indicated in severe cases. Prognosis is generally good, with inflammation often resolving as the immune system matures and consistent dental care is maintained.

Feline hyperplastic juvenile gingivitis (right upper jaw).

Feline hyperplastic juvenile gingivitis (same cat, left upper jaw).
Feline Juvenile-Onset Periodontitis
Feline juvenile-onset periodontitis is an aggressive and uncommon condition affecting young cats shortly after permanent dentition eruption. The disease is characterized by rapid periodontal attachment loss that is disproportionate to plaque accumulation, likely due to an abnormal host immune response. Clinical signs include gingival inflammation, early halitosis, tooth mobility, and oral pain at a young age. Management requires early and aggressive intervention with professional dental therapy and extraction of teeth with poor prognosis. Long-term outcomes are guarded, as many cats require multiple extractions over time, but quality of life can be maintained with appropriate care.
Feline Alveolar Osteitis (Alveolar Bone Expansion)
Feline alveolar osteitis, also known as alveolar bone expansion, is a chronic proliferative condition of the alveolar bone associated with long-standing oral inflammation. Sustained inflammatory stimuli resultin abnormal bone remodeling characterized by diffuse bone expansion and sclerosis rather than bone loss. Clinically, cats may present with firm jaw enlargement, facial asymmetry, and varying degrees of oral discomfort, though some cases are incidental radiographic findings. Treatment is supportive and aimed at controlling underlying dental disease through extractions, dental cleaning, and pain management. While complete resolution is uncommon, disease progression can often be slowed, allowing affected cats to maintain acceptable quality of life.

Alveolar osteitis. Notice pronounced bulging appearance of the osseous tissue (bone expansion) at the upper canine tooth.

There was a significant periodontal pocket around this tooth, therefore the canine tooth was extracted.
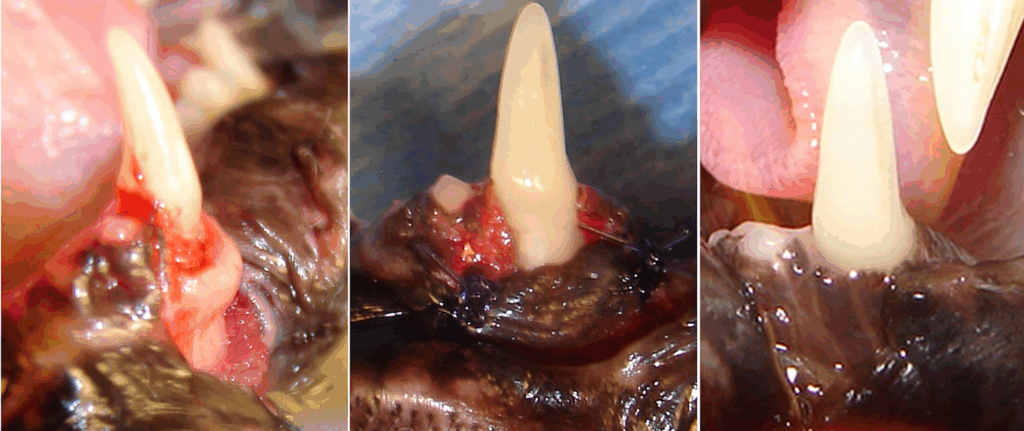
This mandibular canine tooth had alveolar bone expansion (alveolar osteitis) and bony pocket around the tooth. To save this tooth, a buccal mucoperiosteal flap was raised and the irregular crestal alveolar bone was resected and re-contoured. Flap was apically repositioned and sutured. At three-month recheck alveolar osteitis and periodontal disease were gone and the tooth appeared healthy.
Feline Eosinophilic Granuloma Complex
Feline eosinophilic granuloma complex is an immune-mediated inflammatory condition often associated with hypersensitivity reactions. Feline indolent ulcers most commonly develop on or around the upper lips and initially appear as small erosions that may gradually enlarge into ulcerated, swollen, and potentially disfiguring lesions. Despite their appearance, they are typically not painful or pruritic. Feline eosinophilic plaques usually occur on the abdomen or medial thighs and present as raised, well-demarcated, erythematous lesions that may be large, ulcerated, and intensely pruritic. Feline eosinophilic granulomas are most often found on the thighs, face, or within the oral cavity and appear as firm, well-circumscribed nodular or linear swellings on the skin. Oral lesions manifest as raised white-to-pink nodules or plaques on the tongue or palate and are typically non-pruritic.Management typically involves corticosteroids or other immunosuppressive therapies, along with identification and control of underlying allergens. Prognosis is generally favorable, although relapses are common and long-term management may be required.

Indolent ulcer on the upper lip.

Eosinophilic granuloma on hard palate.